

AAV-mRENIN Induced Hypertension Model
Hypertension is a cardiovascular syndrome characterized primarily by elevated systemic arterial pressure, classified into primary hypertension and secondary hypertension. Primary hypertension accounts for over 90% of cases, with its etiology remaining unclear and associated with multifactorial interactions including genetic and environmental factors (e.g., high-salt diet, obesity, and mental stress). Secondary hypertension is caused by specific underlying diseases. The pathogenesis involves abnormalities in neural regulation, renal dysfunction, and vascular structural changes. Epidemiological studies indicate that the prevalence of hypertension increases with age, with a global prevalence rate of approximately 30%-40%.
The renin-angiotensin system (RAS) regulates blood pressure and fluid balance by catalyzing the conversion of angiotensinogen (AGT) to angiotensin I (Ang I) via renin, which is then transformed into angiotensin II (Ang II). Overexpression of murine renin using AAV in mice excessively activates the RAS system, leading to elevated blood pressure. Continuous monitoring of blood pressure is performed using the non-invasive tail-cuff method, and pathological analysis of vascular remodeling is conducted using H&E staining.
B6J mice injected with AAV-mRENIN exhibit elevated blood pressure, increased UACR (urine albumin-to-creatinine ratio), and thickened vascular walls. After four weeks of treatment with the standard of care drug, Lisinopril, significant improvements can be observed in blood pressure, UACR, and vascular remodeling.
Example Data
1. Study design.
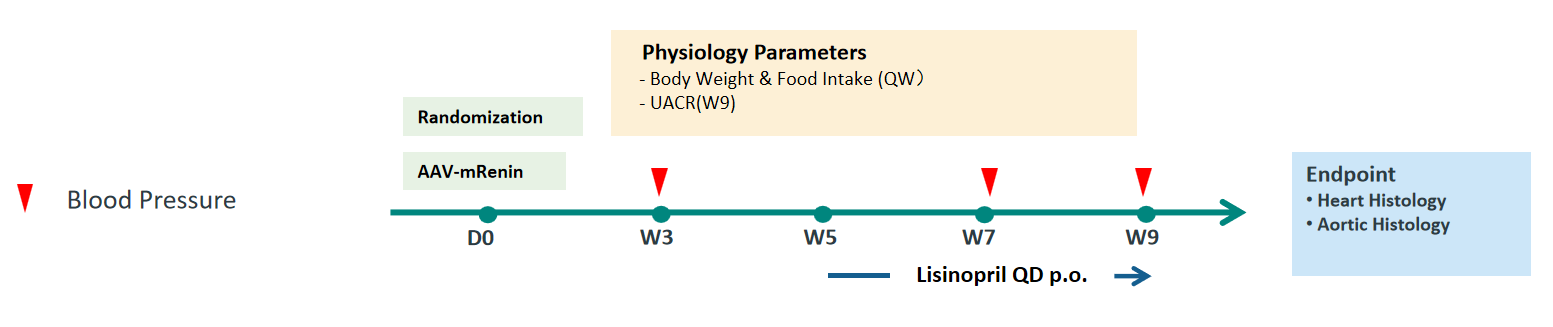
Figure 1. Study design. Typical studies run for approximately 9 weeks with repeated measures for blood pressure, body weight, food intake, and UACR.
2. AAV-mRENIN induction leads to elevated blood pressure in mice.
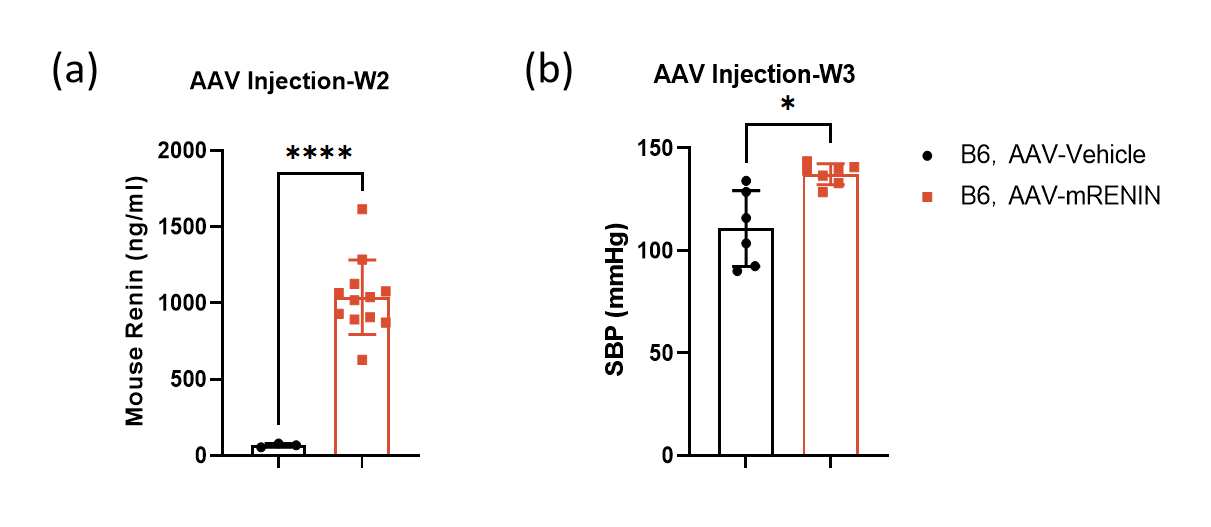
Figure 2. Mouse renin level and systolic blood pressure. (a) Two weeks after AAV injection, plasma renin levels were measured by ELISA. (b) Three weeks after AAV injection, systolic blood pressure in mice was measured using the non-invasive tail-cuff method. (Data are presented as Mean±SD, n = 6-12 per group,*,****denoted p<0.05,p<0.0001, respectively).
3. Lisinopril ameliorates AAV-mRENIN-induced elevation in blood pressure and vascular remodeling.
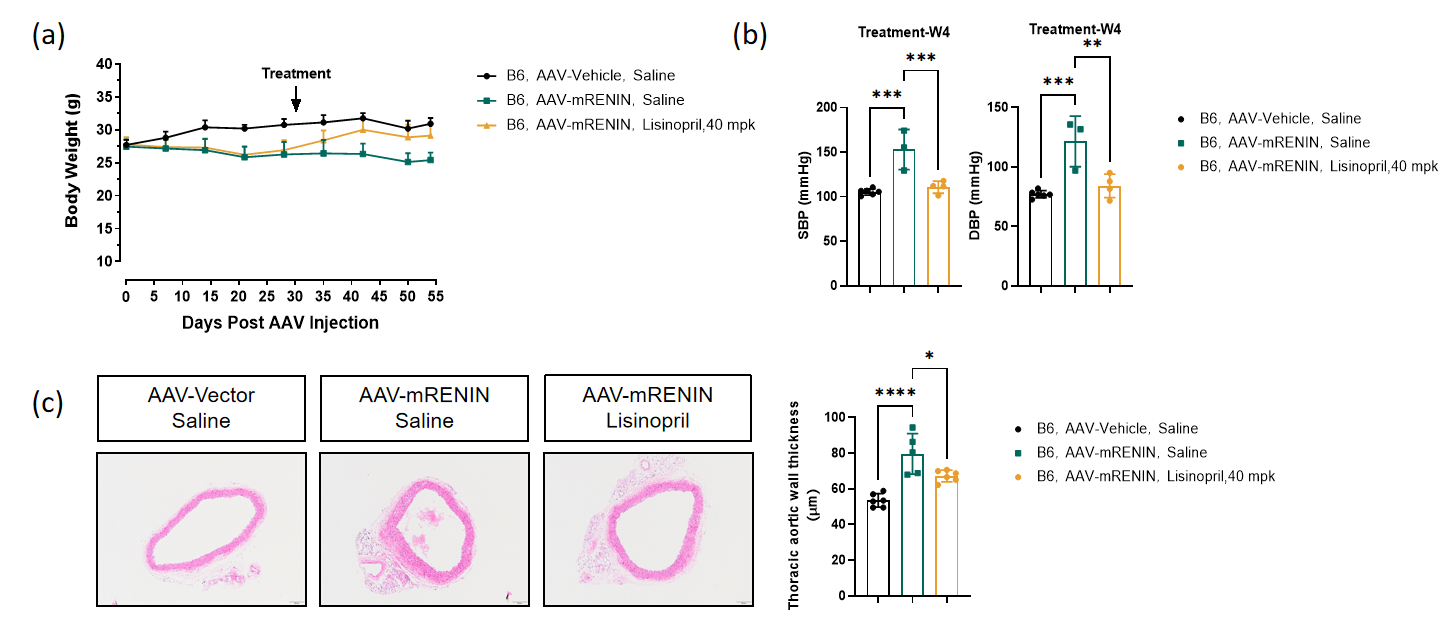
Figure 3. (a) After AAV injection, the mice exhibited weight loss, and their weight began to recover following the initiation of Lisinopril treatment. (b) After four weeks of Lisinopril treatment, the blood pressure of the mice decreased. (c) After four weeks of Lisinopril treatment, the vascular wall thickness of the mice decreased. (Data were presented as Mean±SD, n = 5-6 per group, **,***,****denoted p<0.01,p<0.001,p<0.0001, respectively).
4. Perivascular fibrosis around the heart vessels following four weeks of Lisinopril treatment.
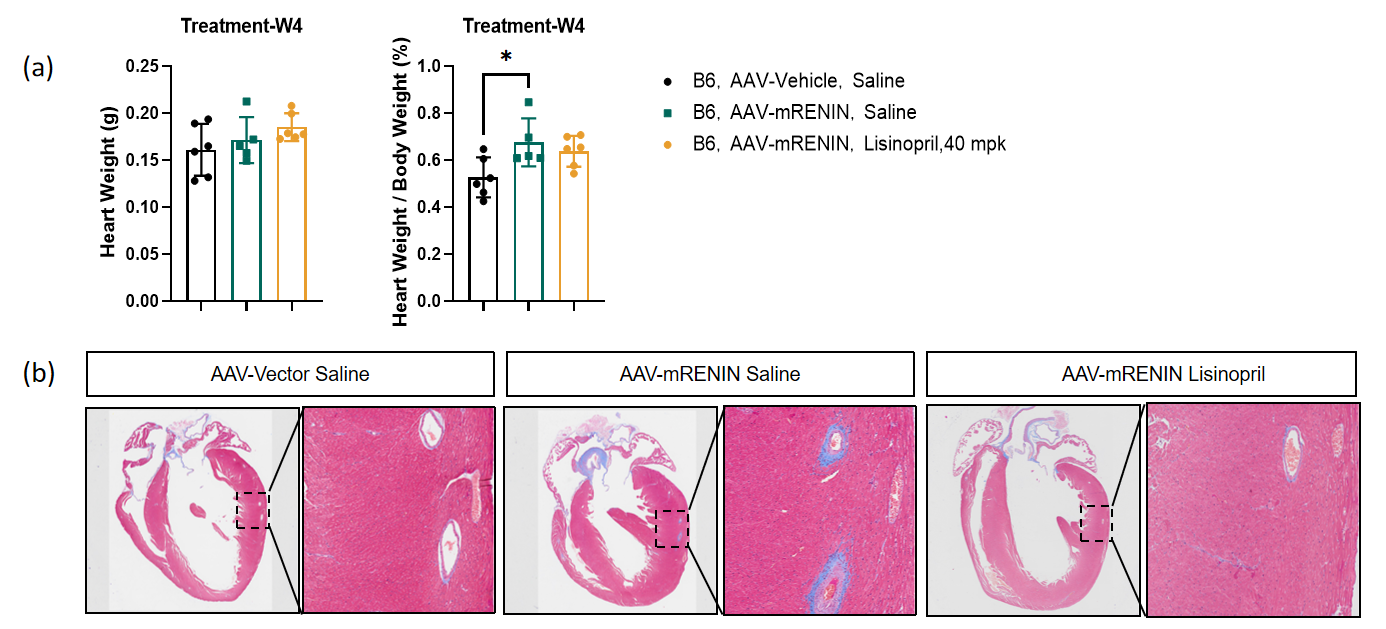
Figure 4. (a) Heart weight. (b) Heart Masson Staining. (Data are presented as Mean±SD, n = 5-6 per group, * denoted p<0.05).
5. Assessment of kidney function following AAV-mRENIN and Lisinopril treatment.
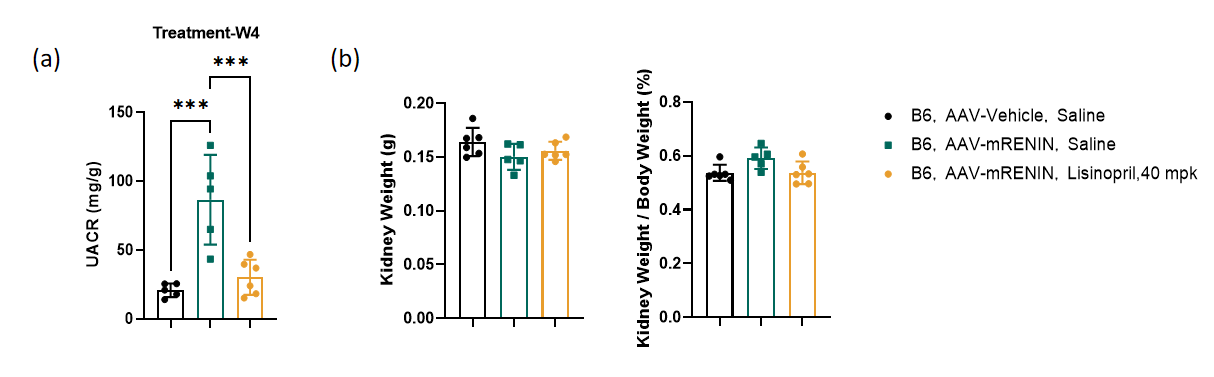
Figure 5. (a) UACR level. (b) Kidney weight. (Data were presented as Mean±SD, n = 5-6 per group, *** denoted p<0.001).